
26 Feb You’re Pregnant! That’s Something to Smile About
It seems to get more and more complicated to be a mother nowadays. Information for pregnant women is so accessible and we feel empowered to make better decisions for ourselves and our little ones. But in reality, most of the information we dig up can be conflicting advice that only leaves us more confused.
When we are uncertain how to proceed, we often defer to our natural instincts and gravitate towards making a safe decision. For expecting mothers who are not sure if a dental visit will be safe for your baby, it can be easy to postpone your regular dental visit. But what are the consequences of ignoring your dental health?
When a mother is healthy, there are relatively few complications of pregnancy that arise from poor oral hygiene. However, due to the hormonal changes that occur during pregnancy, expectant mothers may experience bleeding gums despite maintaining the same brushing routine.
The increased bleeding in the gums (pregnancy gingivitis) can lead to gum disease which is linked to an increased risk of low birth weight and premature birth.* (Studies have shown that this link may exist, but is not definitive). It is a good idea to schedule a dental visit so that all the plaque and tartar build-up can be thoroughly removed.
Some pregnant women also experience a hypersensitive gag reflex and morning sickness, which will contribute to enamel erosion and bad breath. The enamel erosion may cause cavities to form and if not treated, will lead to dental infections. This is problematic because most medications pose some degree of risk to the developing fetus; therefore, it is extremely important to prevent any of these problems from occurring.
The majority of fetal development occurs during the first trimester. It is the period in fetal development with the greatest chance of malformation; therefore, it is generally not advisable for mom to undergo elective dental treatment at this time. However, dental emergencies should still be treated. Your dental provider should be informed of your condition so they can adjust their treatment accordingly.
The second trimester is the safest period to undergo routine dental treatment.
Your dental provider will use this appointment to control any active disease, such as excessive gingival bleeding and cavities, to prevent potential problems from occurring in the late stages of pregnancy and after delivery. Although dental radiographs pose very little risk to the developing fetus, they are still generally not used during this dental visit.
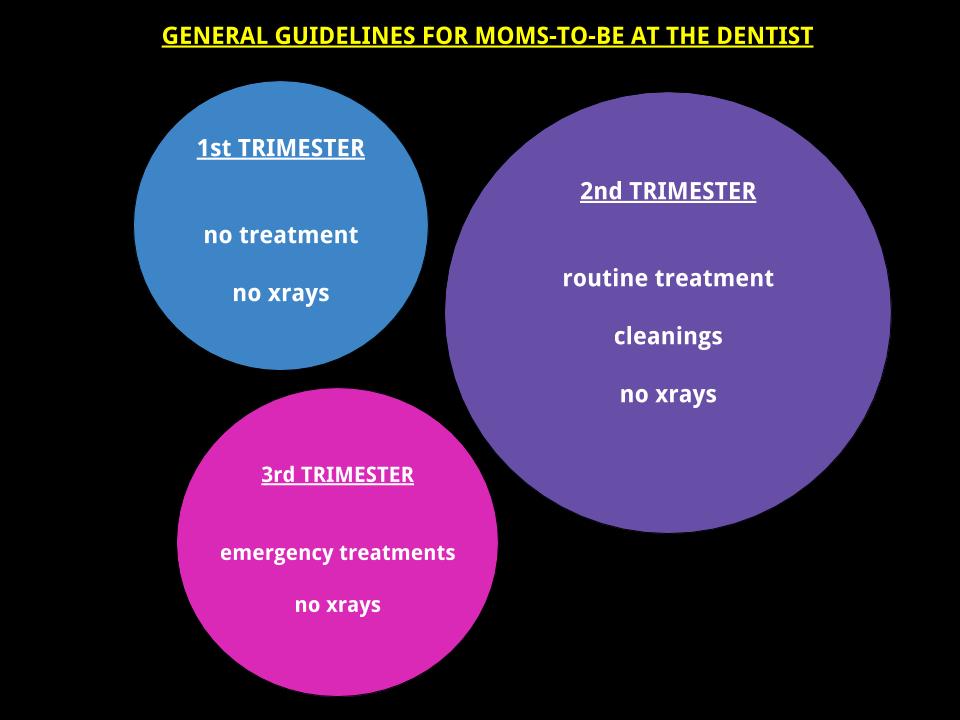
Pregnant mothers in their third trimester should postpone any elective dental treatment because of the discomfort from sitting in the dental chair. Although this is may not apply to everyone, it is general guideline to help avoid patients from experiencing a drop in blood pressure from lying in a dental chair for too long.
In conclusion, routine dental care is encouraged during pregnancy to help expectant mothers maintain good oral health and avoid problems that may not be easily treated without posing risks to your developing baby. Your dental office would love to help you make this stage of your life as comfortable and healthy as possible.
Tips for Maintaining Good Oral Hygiene During Pregnancy
Try using a power toothbrush with a smaller brush head to avoid a gag reflex. Or use a baby toothbrush if that’s all you can tolerate.
Switch to a toothpaste with higher fluoride content (Ex. PreviDent) to help combat cavities. Please remember to spit out the toothpaste and rinse thoroughly.
Rinse with warm tap water after experiencing morning sickness to rid your mouth of stomach acid that can decay teeth and cause bad breath.
Talk to your dentist about anti-microbial rinses to help reduce gingivitis. Avoid alcoholic rinses because they will dry out your gums and cause more gingival irritation.
Floss everyday. It has to be said because it is important. The majority of cavities start from between the teeth where it is not accessible by a toothbrush.
* Offenbacher S, Lieff S, Boggess KA, Murtha AP, Madianos PN, Champagne CM, and others. Maternal periodontitis and prematurity. Part 1: Obstetric outcomes of prematurity and growth restriction. Ann Periodontol 2001; 6(1):164–74
Michalowicz BS, Hodges JS, DiAngelis AJ, Lupo VR, Novak MT, Ferguson JE, and others. Treatment of periodontal disease and the risk of preterm birth. N Eng J Med 2006; 355(18):1885–94